
Case Published: July 2018
Diagnosis: Adenovirus nephropathy in a kidney allograft
Case Summary: Tricky case! Here we have a patient with a kidney transplant, recent treatment of acute cellular rejection (ACR) with T-cell depleting immunosuppression, and acute kidney injury. There is no history of poor PO intake and the patient does not respond to a fluid challenge – making pre-renal AKI unlikely. The biopsy shows us significant interstitial inflammation, viral inclusions, adenoviral viremia and adenoviuria, and a IHC stain that is likely positive for adenovirus – making this diagnosis adenovirus nephropathy in a kidney allograft. This patient is particularly susceptible to this process given the recent use of a T-cell depleting immunosuppressive agent.
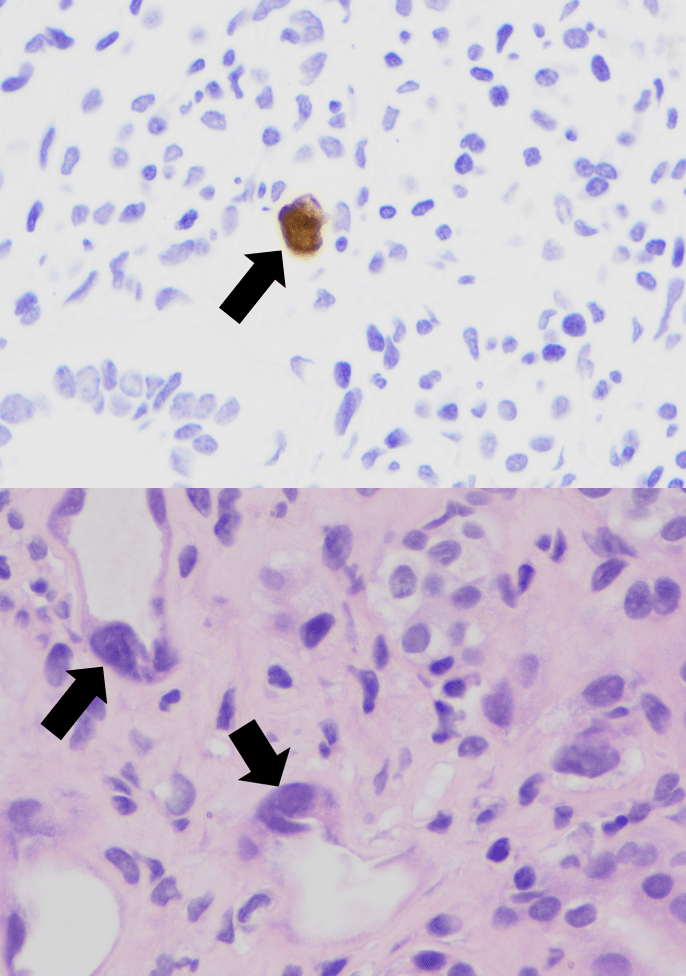
Adenovirus is a double-stranded DNA virus with more than 50 distinct serotypes.Though adenovirus infection is relatively common, adenoviral infection of the renal allograft is rare and also difficult to diagnose if viral inclusions are not present in the biopsy (see image above, black arrows indicating nuclear viral inclusion bodies). Based on a limited number of reported cases, patients typically present with fever, hematuria, dysuria, and acute kidney injury. Adenoviremia and viruria are present, as well as decoy cells similar to those seen with BK virus infection.
Adenoviral infection usually affects multiple organs and can be life threatening, though some patients are able to clear the virus and recover complete allograft function.
Treatment consists of reduction of immunosuppression with or without anti-viral treatment – though these medications, such as intravenous cidofovir, may also be nephrotoxic. Take a look at adenoviral inclusions and IHC stains for adenovirus below:
Case 12 Index
Case 12 Introduction
Case 12 Physical Exam
Case 12 Diagnostic Testing
Case 12 Pathology
NephSim