
Case Published: December 2021
Case Submitted By: NephSIM Nephrons Tubule 11: Distal Convoluted Tubule (2021)
Trainees: Albert Bui, Harsha Adnani, Alessandra Tomasi, Megan Chalupsky, Mario Suito, Carmen Cajina, Vipin Varghese
Faculty Mentors: Matthew Sparks, Meera Harhay, Roslyn Mannon
Diagnosis: Heme Pigment-Induced Nephropathy
Case Summary: Great work! Let’s review this case.
In this case, a 49-year-old woman with a history of cavernous hemangiomas presented with an acute kidney injury (AKI) after undergoing radiofrequency ablation (RFA) of a hemangioma. Despite isotonic fluid administration and Foley catheter insertion (making bladder outlet obstruction less likely), her creatinine continued to rise – making volume depletion less likely as a culprit. Initial laboratory data revealed a hemoglobin of 9.5 g/dL (normal baseline 2 weeks ago) and total bilirubin of 1.7 mg/dL (normal: 0.3 – 1.2 mg/dL). Urinalysis revealed large “blood”, without evidence of significant hematuria. Interestingly, the supernatant appeared red after centrifuge (rather than the usual clear or yellowish color) – raising suspicion for hemoglobinuria or myoglobinuria. A normal creatine phosphokinase (CPK) makes myoglobinuria and rhabdomyolysis unlikely, so let’s shift our attention possible causes of hemoglobinuria…
Our laboratory data support ongoing hemolysis (anemia, hyperbilirubinemia, elevated lactate dehydrogenase (LDH), and undetectable haptoglobin). We also see schistocytes (i.e. “helmet cells”) on the peripheral smear which also suggest hemolysis. A urine hemoglobin test confirms hemoglobinuria. Though it’s possible that the contrast and ketorolac administration may have contributed to the AKI, heme pigment-induced injury is likely to be driver of AKI here given our data. How does hemoglobin injury the kidney? The mechanisms are similar to myoglobin-induced injury described in Case 4 (AKI due to rhabdomyolysis). Both myoglobin and hemoglobin contain heme pigments.
2. Release of ferrihemate from hemoglobin/hemoglobin-induced oxidative injury increases vasoconstriction, decreases vasodilation, and ultimately leads to tissue ischemia and direct tubular toxicity. Recent studies have also shown that iron liberated from hemolysis may trigger the NLRP3 inflammasome and subsequent generation of inflammatory cytokines
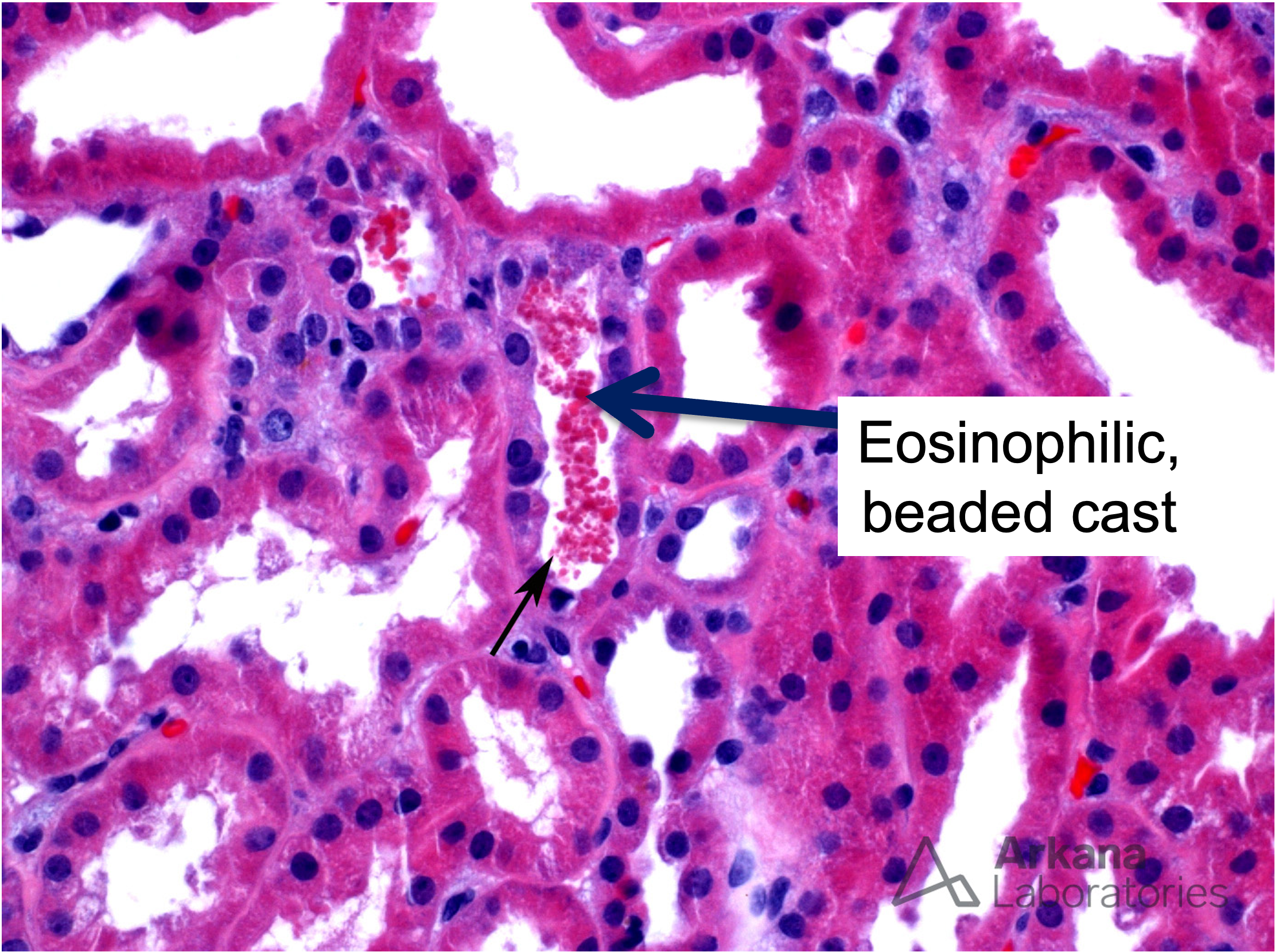
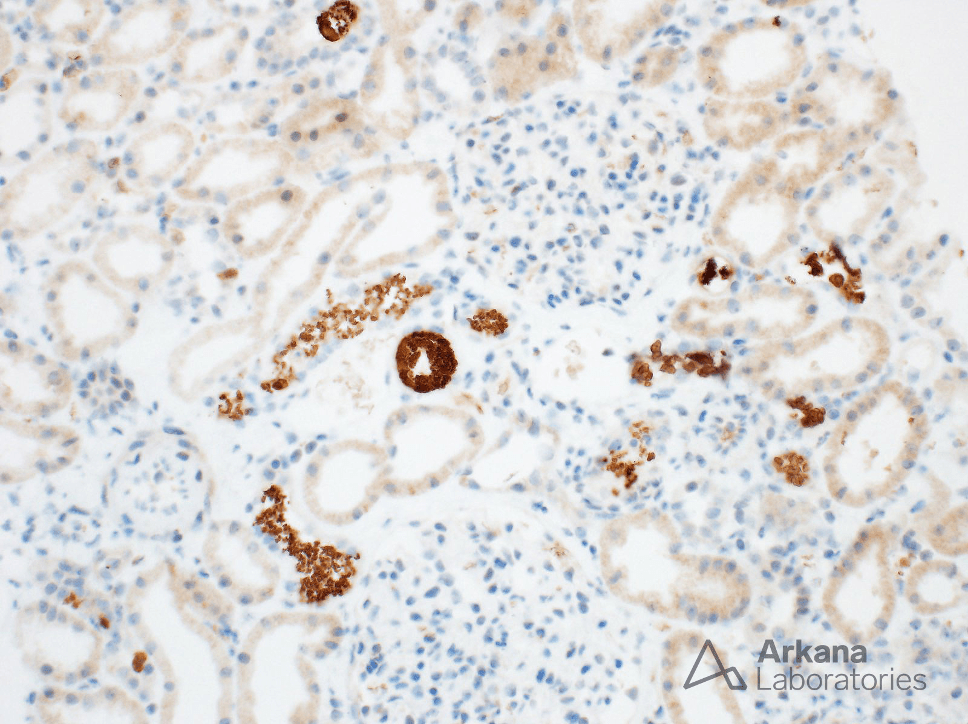
3. Tubular obstruction due to hemoglobin casts (hemoglobin + Tamm-Horsfall protein)
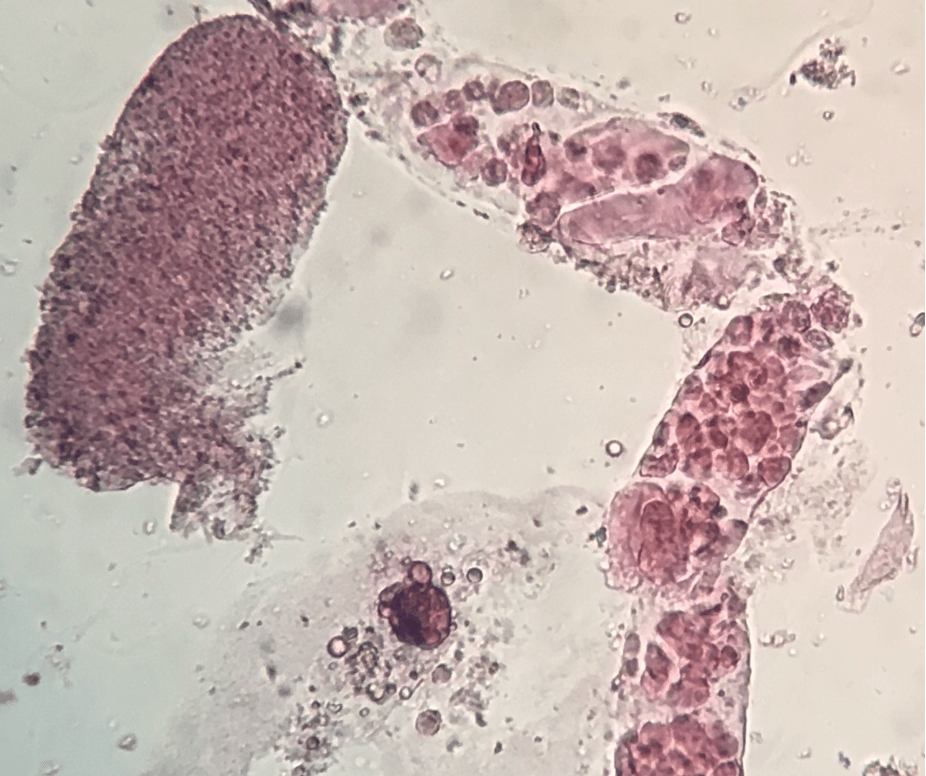
Below is a picture of a hemoglobin cast (Magnification: 400X; Left: Bright field microscopy; Right: Phase contrast microscopy; Courtesy of Jose Tesser Poloni) and accompanying Renal Fellow Network post:

Here’s a Sternheimer-Malbin stained image (left: granular cast; right: renal tubular epithelial cell; 400X; courtesy of Vipin Varghese) suggestive of acute tubular necrosis:
So the cause of AKI here is likely heme-pigment induced nephroapthy. But why? Let’s take a minute to talk about the RFA. During an RFA, a needle is inserted into tissue and radiofrequency waves are sent from the probe into the surrounding tissue and the temperature of this tissue can reach 122 -212°F. That’s hot! Red blood cells may undergo “thermal hemolysis” at temperatures greater than 120°F – and thus RFA of large hemangiomas may result in massive hemolysis. Heme pigment-induced nephropathy is an uncommon yet significant potential complication following RFA.
Though biopsy isn’t needed to make the diagnosis here, let’s take a look at what we might see:
Fortunately, our patient showed recovered kidney function with supportive care (including a few weeks of dialysis). Peri and post-operative fluid resuscitation may prevent heme pigment-induced AKI in patients undergoing RFA.
Case Published: December 2021
Case 53 Index
Case 53 Introduction
Case 53 Physical Exam
Case 53 Diagnostic Testing
NephSIM