
Take a look at some initial diagnostic testing below.
Urinalysis/microscopy, urine electrolytes
Basic labs
Kidney Ultrasound

Choose 3 of the most high yield tests below!
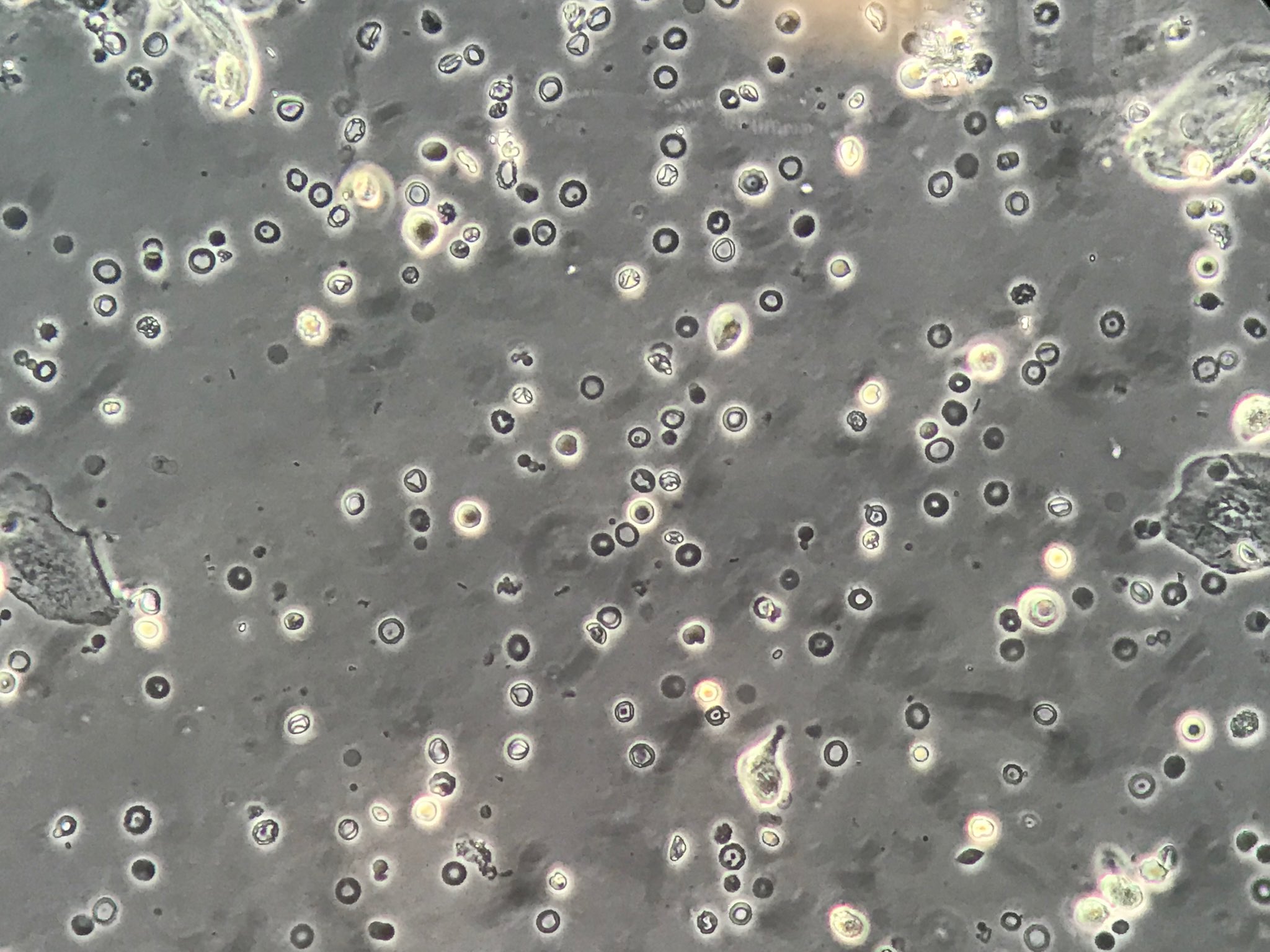
Urine sediment
Excellent choice! Hematuria should be differentiated as glomerular or non-glomerular if possible, by looking at the urine sediment. What do you see?
Anti-nuclear cytoplasmic antibody (ANCA) levels
Antibodies against proteinase 3 and myeloperoxidase are not detected . Though ANCA-associated vasculitis typically presents as a rapid progressively glomerulonephritis (RPGN) and affects individuals older than 50 years old, it can occur at any age and may present with a nephritic syndrome.
Anti-nuclear antibody (ANA) titer
The titer is 1:32.
Complement levels (C3, C4)
Excellent choice. C4 is 20 mg/dL (normal: 16 – 48 mg/dL). C3 is 40 mg/dL (normal: 80 – 160 mg/dL).
Hepatitis B Virus (HBV) & Hepatitis C Virus (HCV) Serologies & PCR
Antibodies against and serum viral loads of HBV and HCV are undetectable.
Urine eosinophils
This is a low yield test here. Traditionally, this test has been described for acute interstitial nephritis (AIN) – though the sensitivity and specificity for AIN is also poor.
Cystoscopy
Before moving to an invasive test like this one, we should try to find out whether the hematuria is glomerular or non-glomerular. The cystoscopy would let us look for a bladder malignancy, which might cause non-glomerular hematuria. Let’s try a higher yield test!
Creatine phosphokinase (CPK)
The CPK can be markedly elevated in patients with rhabdomyolysis, or breakdown of muscle that can subsequently lead to acute kidney injury. Classically, the urine of these patients is positive for “blood” on the urine dipstick, without the presence of red blood cells. Here, we have numerous red blood cells.
Bone marrow biopsy
You consult your hematology colleagues and they advise against a bone marrow biopsy as there are no significant complete blood count (CBC) abnormalities. They advise other diagnostic tests to help this patient.
Anti-phospholipase A2 receptor antibody level
We might order this test in a patient with nephrotic syndrome to look for primary membranous nephroapthy. Given the findings so far, this is a low-yield test here. Try again!
Update your differential diagnosis before moving on! (choose 3)!
Membranous nephropathy
Bladder cancer
Diabetic nephropathy
C3 glomerulonephritis
Acute interstitial nephritis (AIN)
ANCA-associated glomerulonephritis
Systemic lupus erythematosus (SLE) nephritis
Dense deposit disease (DDD)
Acute tubular necrosis (ATN)
IgA nephropathy
Hepatitis C-related glomerulonephritis
Hepatitis B-related glomerulonephritis
Click here to perform the biopsy!
Case 43 Index
Case 43 Introduction
Case 43 Physical Exam