
Take a look at some initial diagnostic testing below.
Urinalysis/microscopy, urine electrolytes
Urine sediment
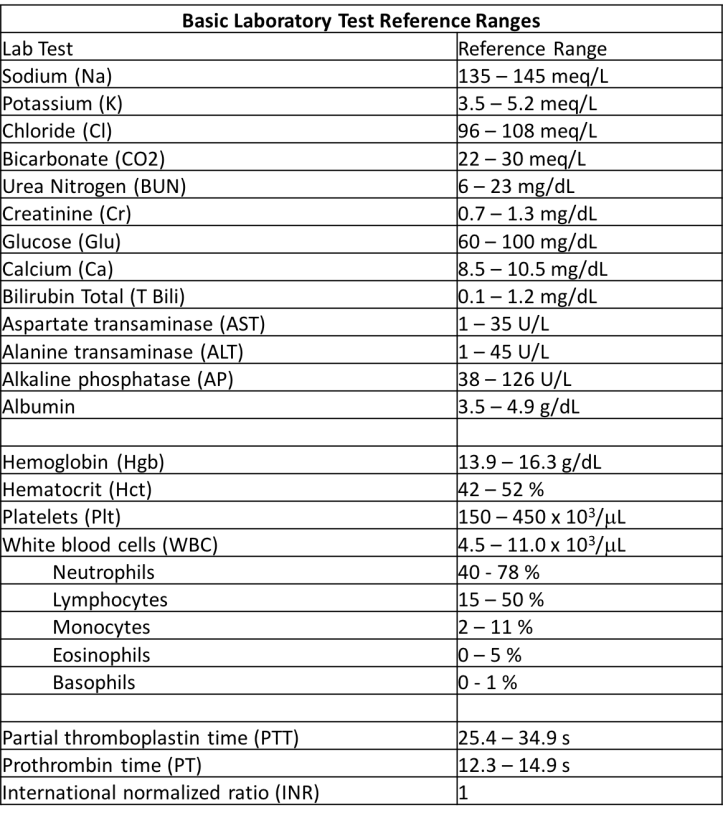
Basic labs 
Kidney Ultrasound
Choose the highest-yield tests below (multiple tests may be correct)!
24 hour urine collection for protein quantification
Correct! Though the urinalysis did not pick up proteinuria, we should investigate the possibility of non-albumin proteinuria. The 24 hour urine collections reveals 6 g of proteinuria.
Complement levels (C3, C4)
Not the highest yield test here, the patient’s urine sediment and urinalysis do not suggest a nephritic syndrome. The complement levels are normal.
Hemoglobin A1C
If we’re thinking about diabetic nephropathy, we would likely see albuminuria picked up by the urinalysis. Let’s try again!
Intact parathyroid hormone (iPTH) level
Excellent – we should check the iPTH level in a patient with hypercalcemia. The level is undetectable here.
Urine culture
Without pyuria, leukocyte esterase in the urine, or symptoms of a urinary tract infection, the urine culture is unlikely to provide us with information to help with this case. Choose again!
Urine eosinophils (Hansel’s stain)
This test with poor both sensitivity and specificity had been traditionally used to look for AIN. Regardless of the patient’s history and labs, this test is not high yield. Pick again!
We have a lot of data! what are the top three diagnoses on your differential?
Myeloma cast nephropathy
Systemic lupus erythematosus (SLE) nephritis
Light chain deposition disease
Amyloidosis
Post-infectious glomerulonephritis
Membranoproliferative glomerulonephritis
IgA nephropathy
Acute interstitial nephritis
Obstructive uropathy
Hypertensive nephropathy
Light chain proximal tubulopathy
Heavy chain deposition disease
Focal segmental glomerulosclerosis (FSGS)
Click here to move on to the kidney biopsy!
Case 21 Index
Case 21 Introduction
Case 21 Physical Exam